

Are Mental Health Professionals Perpetuating Stigma Around DID?
Are Mental Health Professionals Perpetuating Stigma Around DID?
It's Time For Change


Stigma & Stereotypes
It’s no secret that we have strong feelings about stigma and the need for it to end. Regardless of a person’s diagnosis or struggle, stigma and stereotyping are often enormous barriers to care, and that fact threatens lives. Addictions, Bipolar Disorder, Eating Disorders, Borderline Personality Disorder-actually all personality disorders- are all highly stigmatized. And then there’s DID/OSDD which comes with it’s own special kind of hellish stigma. If you’re not deemed completely crazy, you’re thought of as akin to a dangerous serial killer. Hey, thanks, media!…or, lately, more often than not, you might simply be written off as “faking it, because we don’t believe DID exists.”
I’m sorry, what?
That’s right. There is a whole slew of folks out there who don’t believe DID exists at all, despite the fact that it has been observed for hundreds of years across every culture and continent. Then there is an equally large group of people who clutch onto the damaging belief that the people who live with DID are merely ‘faking it,”…because apparently, what? They have nothing better to do?
There are so many ways in which DID is stigmatized. On the one hand, when it comes to the general uninformed public, we get it. Informed only by Netflix and HBO movies, where violence and psychological thrillers sell, it makes sense that the general public might end up with a completely skewed concept of what DID is. Fiction is their only context. But what about the mental health professionals who many people believe “should know better?”
Let’s pause for a moment to acknowledge that there are many mental health professionals who do compassionately support and treat people living with DID. There are providers who not only “believe in it,” but who know how to deliver expert care that facilitates genuine healing. This blog is not about that talented minority. We appreciate them more than words can say. This blog is about the rest.
Looking up at that last paragraph, it feels odd to write the phrase, “there are providers who not only ‘believe in it,’” because words like “believing in” the existence of something are better reserved for conversations about Santa Claus with questioning children rather than an entire diagnosis that results from chronic, severe childhood trauma. But… here we are. How did we even get here?

The Background
In graduate school, nearly everyone is taught that “DID is so rare, you’ll never see it. Don’t worry about it.” It is glossed over in far less than 15 minutes, if it is even addressed at all. In contrast, in our own course of study we spent significant time learning about the various types and presentations of schizophrenia. The professor also took great pains to teach us plenty about various presentations of bipolar disorder, including the difficult to spot rapid cycling bipolar II. The class was captivating, the professor talented, and, as a result, we all became pretty good diagnosticians. In our case, we’ve been able to identify diagnoses that seasoned psychiatrists missed in several settings we’ve worked in. You might be thinking that nothing is amiss. That makes sense. Of course we’d all get training in diagnoses as well known as schizophrenia and bipolar disorder!
Let’s look at the numbers.
NAMI estimates that in the US the incidence of schizophrenia is between 0.25%-0.65%1 while the WHO puts it at 0.32%2 globally. Still other organizations place the global incidence at around 0.7% and others place it at roughly 1%3…perhaps they are rounding up. The global incidence of Bipolar Disorder is 0.51%4. DID, by contrast, has a global incidence of 1.1 to 1.5%5 For a broader discussion of DID statistics Dr. Bethany Brand’s Separating Fact From Fiction: An Empirical Examination of Six Myths of Dissociative Identity Disorder is worth a read.
The math is pretty simple. The rate of DID exceeds the rate of schizophrenia and bipolar disorder combined.
What gives? Why is it that graduate schools spend plenty of time on both schizophrenia and bipolar disorder, but virtually no time on DID when the rates of DID exceed those of the other two disorders combined? Good question.
Recently on Lisa Danylchuk’s podcast, Dr. Bethany Brand postulated that DID as a diagnosis is doubted due to who the victims are: people who suffered horrific abuse as young children and, to paraphrase, “nobody wants to think about that.” She also noted, if memory serves, that coming out of the False Memory Syndrome (FMS) era, that people in high places had vested interests in both silencing and discrediting victims in order to conceal their criminal behavior. In this same podcast, Dr. Brand notes that she has reviewed psychology textbooks and found that there are many that propagate myths about DID. This results in new professionals lacking the training to identify and treat people with DID. All of this overtly harms people with DID diagnoses. Is it any wonder, then, that those with DID have often gone through 6-10 years of misdiagnoses and ineffective treatments? Is it any wonder that when they do receive an accurate diagnosis that they then have profound difficulty locating a provider who can, or is willing to treat them?
Such. A. Mess.
As someone, who received a DID diagnosis after going through 6 years of many misdiagnoses coupled with some very traumatizing experiences in treatment all during the height of the FMS era, I/we can assure you that the harm caused by the lack of ability on the professional side is more than just significant. Bear in mind, 6 years is actually on the low side to receive an accurate diagnosis. Technically, we’re one of the “lucky” ones.
Continued Controversy
“It doesn’t exist” “DID is just a fad” “It’s over diagnosed” are all sentiments heard throughout the mental health profession. Yet, these sentiments do not reflect what we know from research.
The first published case of DID was that of Jeanne Fery in 1586.6 Cases of DID have continued to be reliably identified, diagnosed and documented throughout time and across every continent.7 Dr. Bethany Brand and colleagues conducted a review of studies that used systematic assessments and structured interviews to diagnose DID. The studies are summarized in her table here:
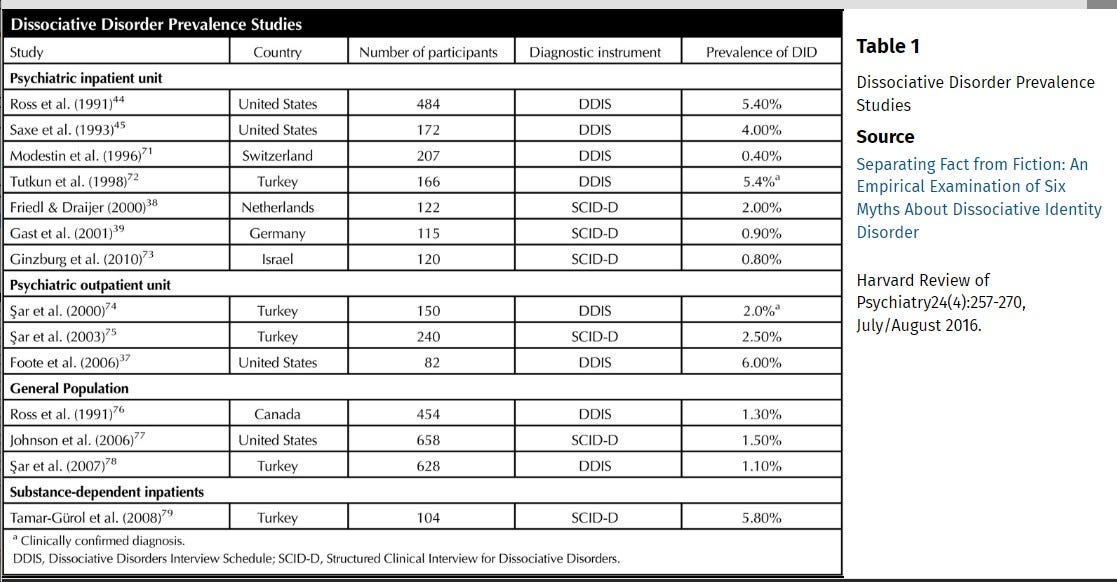
Not only do these studies prove the existence of DID (and we hate having to even say that, because that shouldn’t even be a thing!! We don’t spend time trying to prove the existence of any other disorder in the DSM besides DID), but these studies also exemplify the diverse continents that people with DID are found on: Canada, Germany, Israel, the Netherlands, Switzerland, Turkey, and the United States. Now, you might be thinking that seven countries are still a limited representation of the global prevalence, and, if you happen to be a doubter, you might also be thinking “big hairy deal.” Hold up. Dr. Brand cites another prospective study that assessed treatment outcomes of DID patients from around the world. In this study literally every single continent except for Antarctica was represented.8
DID exists. It’s certainly not rare when compared with schizophrenia and bipolar disorders. And, despite McLean’s March Grand Rounds Presentation (see our analysis of that here) that suggested the existence of a plethora of “imitative DID” by pilfering the content of people who were actually professionally diagnosed with DID; DID is real, it exists and it’s everywhere.
Professionals and Their Feelings
We apologize if the subheading above sounds snarky. It’s not meant to.
Some professionals do have feelings about DID, and they can be pretty vocal about them. “I don’t feel comfortable about DID diagnoses.” “I have mixed feelings about DID.” “I don’t feel like DID is actually real.” “I feel like people with DID are just being dramatic and theatrical.” First things first. Those last two sentiments are thoughts y’all, not feelings. Just sticking the word “feel” in the sentence doesn’t make it a feeling. But we digress.
Here’s the thing, given that professionals have received such little training on DID, it makes sense that they might have some questions, thoughts and feelings. We wonder, though, why many professionals haven’t thought to dig into the literature at least a little bit rather than dismiss DID with an abrupt, “Oh, I don’t treat that.” Mmmkay, but given the statistics you probably do and just don’t recognize it. That situation isn’t good for the therapist or client.
Given the recent controversy (referring to the ISSTD panel and McLean’s Grand Rounds in March) you’d think more therapists would seek training in complex dissociation, DID in particular, and wonder why it is that they haven’t been adequately trained in it. Lack of training and exposure to media coupled with lack of self awareness has some providers perpetuating myths associated with DID, e.g. that we’re all dangerous, will never heal, and will never be able to function. All of this couldn’t be further from the truth, by the way.
We’ve overheard many, many providers essentially ‘shit talking’ people with DID, suggesting that they’re ‘bad actors,’ ‘attention seeking,’ or worse, “outright lying.’ We’ve heard them making off handed comments about people with DID, as well as using DID as a way of denigrating someone else by saying things like “Oh she’s so DID,” accompanied by an eye roll. We’ve been in staff rooms and conferences that are rife with derogatory DID related jokes. Disgusted to learn this? Most of them don’t think they’re doing anything wrong. Many will tell you that they believe that they are compassionate, good therapists and that this kind of “blowing off steam” isn’t harmful. Except that it is. It perpetuates stigma, stereotypes and shame, and every last therapist with a license is ethically responsible to do better.
People with DID are some of the most vulnerable people in society, who have suffered the most horrific, unspeakable traumas. The last thing anyone with DID deserves is to be on the receiving end of more judgment, insensitive jokes and poor care. It’s inconsiderate at best, damaging at worst.
Maybe We’re Just… Angry?
Human behavior is complex and professionals are not exempt from this fact. At the same time, we expect more from people who are trained and should ultimately know better. Even if a professional is not trained in complex dissociation, they can at the very least use a strength’s based lens and refuse to engage in any conversation or exchange that denigrates any population of people. That is basic.
Even therapists with multiple related certifications are not exempt from bad behavior that perpetuates stigma. We had a former therapist who had several certifications that made her ostensibly well equipped to treat DID. Yet, we often found ourselves listening to her disparage her other clients with sarcastic comments about their late night dissociative activities. We sat through her looking bored and rolling her eyes when we dissociated. We sat through her making jokes about people who dissociate while frequently forgetting that we were her client, not her colleague. At one point, in a tirade discrediting another well known trauma therapist along with people with DID (seemingly ignoring the fact that we have it, too), she suddenly looked startled. She looked to her right, composed herself, straightened her posture and then looked back at us stating, “I just want to clarify that I’m speaking to you now as a colleague not a client. Colleague to colleague.” In the event anyone is wondering, this is not how individual therapy sessions are supposed to go. That is what it looks like when someone needs consultation and a long vacation.
Systems can be profoundly high functioning. But that doesn’t mean that there isn’t also a great deal of suffering that needs tending to and healing. Systems can also struggle profusely to function at all. And that doesn’t mean there aren’t also parts that are more than capable of functioning beautifully in the world. It’s just that those parts might not be accessible right now. One thing we know for sure: every system is the result of a brain being brilliantly creative in its efforts to successfully survive unspeakable trauma. And that, alone, warrants voluminous compassion and respect.
So, all that said, if you are a therapist who does know much about DID, please begin to educate yourself. If you are a therapist who treats DID, please check in with yourself frequently around your language, belief systems, training being up to date, and compassion for suffering. And thank you for all you are doing for systems everywhere. If you are a system, please know that no matter what anyone anywhere says, you are valid and you have superpowers you probably haven’t even discovered yet. Believe in yourselves. We believe in you.
Middleton W, Butler J. Dissociative identity disorder: an Australian series. Aust N Z J Psychiatry 1998;32:794–804.
Foote B, Smolin Y, Kaplan M, Legatt ME, Lipschitz D. Prevalence of dissociative disorders in psychiatric outpatients. Am J Psychiatry 2006;163:623–9.
Friedl MC, Draijer N. Dissociative disorders in Dutch psychiatric inpatients. Am J Psychiatry 2000;157:1012–3.
Gast U, Rodewald F, Nickel V, Emrich HM. Prevalence of dissociative disorders among psychiatric inpatients in a German university clinic. J Nerv Ment Dis 2001;189:249–57.
Horen SA, Leichner PP, Lawson JS. Prevalence of dissociative symptoms and disorders in an adult psychiatric inpatient population in Canada. Can J Psychiatry 1995;40:185–91.
Latz TT, Kramer SI, Hughes DL. Multiple personality disorder among female inpatients in a state hospital. Am J Psychiatry 1995;152:1343–8.
Lewis-Fernández R, Martínez-Taboas A, Sar V, Patel S, Boatin A. The cross-cultural assessment of dissociation. In: Wilson JP, So-Kum Tang CC, eds. Cross-cultural assessment of psychological trauma and PTSD. New York: Springer, 2007;279–317.
Lussier RG, Steiner J, Grey A, Hansen C. Prevalence of dissociative disorders in an acute care day hospital population. Psychiatr Serv 1997;48:244–6.
Ross CA, Anderson G, Fleisher WP, Norton GR. The frequency of multiple personality disorder among psychiatric inpatients. Am J Psychiatry 1991;148:1717–20.
Saxe GN, Van der Kolk BA, Berkowitz R, et al. Dissociative disorders in psychiatric inpatients. Am J Psychiatry 1993;150:1037–42.
Brand B, Classen C, Lanins R, et al. A naturalistic study of dissociative identity disorder and dissociative disorder not otherwise specified patients treated by community clinicians. Psychol Trauma 2009;1:153–71.