

Trauma Informed Care (TIC) in Medical Settings
Trauma Informed Care (TIC) in Medical Settings
TIC Education, a Short Rant & 6 Tips Navigating Them

It feels hard enough to find solid Trauma Informed Care in mental health settings, never mind medical ones. A few recent personal experiences have underscored the ongoing glaring-and highly preventable- issues that arise in so many medical settings. These issues are truthfully challenging enough for singlets; they can be absolutely otherworldly for systems to navigate.
Trauma Informed Care (TIC)1 is intended to be an integral part of service care delivery across multiple healthcare settings. Most professionals receive at least some training in it, and if they haven’t had training in it, they most certainly should get it! Past traumatic experiences negatively impact people in the present day in a variety of ways. Not surprisingly, given the power differentials inherent in medical settings, the impact of past trauma in these settings can be profound. The goal of TIC, then, is to maximize positive outcomes by emphasizing physical, psychological and emotional safety through educating patients about their condition and treatment options, while ensuring they have as much choice as possible over both the care and services they receive. Information is power. Choice is liberating.
In our last job, working for a corporate healthcare giant, we were trained and certified as a TIC trainer. In truth, we really enjoyed training people in how to deliver Trauma Informed Care. Helping people understand the far-reaching impact of trauma felt like we might be making a small dent in an otherwise colossal problem. It was hopeful and even exciting to watch people make connections, see concepts click, and feel the level of compassion they experienced even for the fictitious clients presented in the training scenarios.
In a typical training, attendees are taken through the Adverse Childhood Events or ACE test so they could see their own risk profiles and have an opportunity to think about how their own past experiences impact them. 61% of adults in the US have at least one ACE, though anecdotally in the trainings we gave, it was almost always 100% of participants reporting at least one ACE. Trainees learned about the risk factors associated with higher ACE scores. For example, according to the CDC, ACE Scores of 4 are considered “high” and are associated with an increased likelihood of autoimmune and other chronic diseases. Those with high scores also tend to experience relationship discord and serious mental health issues like depression, suicidality, addiction, and high anxiety. Those with even higher scores are said to be at higher risk for a shortened life span. Trauma is serious (understatement of the century.)
So, how do you translate this information into actual care delivery?
There are all sorts of strategies to help providers remember trauma informed standards of care. The company we worked for used acronyms to help employees in acute care settings follow a basic protocol. The protocol was designed to ensure people feel empowered in their care, regardless of what department they received care from. The acronym reminds them to greet and acknowledge the person immediately upon entering the room as well as to introduce themselves and their position. This immediately communicates to the patient that they are important. It also gives them an idea of the relationship they will have with the person who entered, which helps alleviating anxiety. For example, the relationship you have with the person who is triaging or drawing labs is very different from the relationship you may have with a nurse or doctor. How you mentally prepare yourself for interacting with each of those providers differs.
Once introductions are complete, the employee then describes what will occur during the appointment or encounter itself. This one step is often missed, which is unfortunate, because it is the one that tends to help alleviate anxiety the most. After the description of what will happen, the activities described take place, e.g. an examination. Whether or not an examination happens, the next step in TIC is the salient education about the person’s condition and their treatment options complete with risks and benefits. Following education and treatment options, the provider then encourages the patient to ask questions. Asking, “what questions do you have for me?” tends to increase patient engagement and the likelihood that they will actually ask, rather than using the phrasing “do you have any questions for me?” The former expects and invites questions whereas the latter latently suggests that questions may not be welcome. And last, but certainly not least, the TIC visit closes with the provider thanking the patient upon leaving the room. Thanking the patient reinforces the patient’s inherent importance while conveying respect and genuine gratitude. TIC appointment structures, such as the one outlined here, are designed to disrupt the power differential while ensuring patients have as much agency as possible in their care.

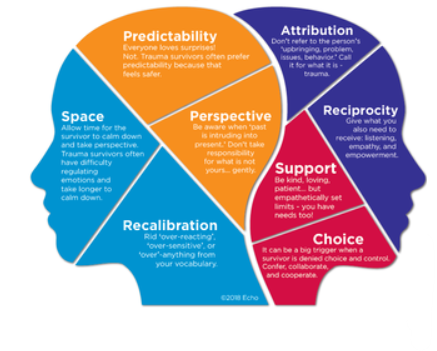
Seeing Through Trauma Glasses
Trauma colors how we experience the world. When a traumatic experience occurs, our frontal cortex (thinking brain) goes offline as our amygdala (fight/flight/freeze/collapse) takes over. Meanwhile, the hippocampus, normally tasked with giving context to memory, downregulates which leads it to tagging things that aren’t particularly salient to the experience itself. For example, if an assailant was wearing a yellow shirt, the hippocampus might tag the color yellow as important. Thus, in the future, as a function of neuroception (the brain constantly scanning the environment for signs of safety and unsafety) the person may become triggered whenever they see the color yellow, even though in the grand scheme of the event itself, the color yellow was inconsequential to the traumatic event itself. Even more disconcerting is the fact that the person may not even know that the color yellow is the trigger.
As you can imagine, triggers abound in virtually any medical settings. Add that to the fact that, due to the downregulation of the hippocampus, people often don’t even know what their triggers are, you have- you guessed it—an absolute minefield (though some of you may prefer the term ‘clusterfuck’ here…but we digress). This combination of unknown triggers coupled with an anxiety provoking environment is precisely why it is important to have trauma informed care in medical settings. Afterall, patients in medical settings are routinely in vulnerable positions physically, mentally and emotionally. Between the condition they are seeking care for, the physical positioning of their bodies and the potential for being triggered by someone in a position of authority, TIC is imperative.
We discovered during trainings that most people, when asked, could easily identify a plethora of ways in which medical appointments could be wildly triggering. They were adept at identifying their possible biases that could negatively impact care. And they were even able to identify simple solutions to mitigate harm to vulnerable people. That all felt encouraging at the time.
Professionally, being a TIC trainer felt satisfying. As a patient who needs to access either routine or sick care, however; the experience has anything but. All of the things that providers and employees had found so easy in the actual training seem to completely confound providers we have seen in practice. Just take these very preventable (and in our opinion obviously harmful) scenarios:
A urologist whose exam room is set up so that the foot of the exam table faces the door. That’s right, all the vulnerable body parts exposed to anyone who opens the door (and anyone in the hall behind them for that matter).
An OB/GYN whose exam table complete with stirrups also faces the door AND a desk and laptop for their ‘scribe’ was placed between the stirrups but back against the wall, making it possible for 3 people to view some very vulnerable anatomy, assuming someone opens the door, which, of course…they did.
Another OB/GYN who seemed adept at TIC by describing everything she was going to do before she did it, said “I’m just going to feel your throat with my hands” while standing behind the body and then blew it by proceeding to wrap her fingers around the neck.
Without warning or discourse, grabbing an arm to take blood pressure.
And, of course, many worse scenarios than these. Is it any wonder trauma survivors find it so hard to attend medical appointments?
The above situations are things that would trigger most all trauma survivors (and possible people without trauma, too). But in the case of people with DID, these situations often cause anything from a switch to rapid switching to going into trance to amnesia. It can happen quickly, and it can last for a period of time throwing the entire system into chaos and upheaval.
It’s kind of infuriating, really. Something as simple as arranging an exam room in a way that is both respectful, compassionate and straight up common sense escapes consideration altogether. It’s baffling that one could engage in enough critical thinking to describe how they will check your thyroid, knowing that that action is likely to startle someone, but still wrap their hands all the way around your neck to do so. All of these things happen even when providers know that the patient has an extensive trauma history. Common sense has left the building. And it’s harmful.

So What Can Be Done??
While it would be nice to just never have to go to appointments, part of this whole overrated adulting thing is attending to the physical body and its health. And, let’s face it, sometimes things come up and we just have to go no matter how much we may not want to.
So, if you are a system and you do need to go to a medical appointment, here are some things that might help:
Prep for the appointment ahead of time. Be sure to make a system announcement that you have <insert specific appointment> on <insert specific date and time.>
Be sure to explain why you need to go.
Ask who might have a difficult time with the appointment.
Ask these parts not to attend the appointment. Ask them to instead do a preferred activity in the inner world. Ask a caretaker part to be with them or nearby and available to them.
Ask even if you don’t know who your caretakers are. Ask even if you haven’t yet established 2-way communication.
Ask who is good at communication, and request that part(s) can be present for the appointment to communicate with the provider. Ask that part(s) to communicate the systems needs upfront at the beginning of the appointment. (e.g. getting weighed vs skipping the weight check; needing a full description of what is going to happen prior to the appointment starting; needing someone to be with you in the appointment; needing to take written notes so you can remember, needing to voice record it on your phone so you can listen later.)
Ask who is good at keeping the body calm and everyone anchored in the present day. Request that part(s) to be present throughout the appointment, working to calm the system.
Ask someone to be responsible for body care both before and after to ensure that you’ve had nutrients, rest and some somatic exercise to regulate the body’s nervous system.
If you feel safe disclosing your diagnosis to the provider, you might consider asking them to watch the short film Petals of a Rose prior to your appointment to help them better understand DID. It has both a full and redacted version and provides education that can help your providers respond compassionately.
The day of the appointment, hold a system meeting to review the plan you made from the questions in part one. Ask if any parts have any questions. Discuss and negotiate any last minute details.
Before leaving consider bringing something that feels comforting to you. It can be something small that fits in your pocket, a phrase that you write on your hand…or maybe a unicorn keychain (since you probably can’t bring a 2-foot unicorn stuffy in with you :) )
On the way to the appointment check in with the part that will be communicating as well as with the part that will be regulating emotions and anchoring you in the present day.
Do your best and know whatever happens is okay.
If you dissociate it’s okay. It’s what you needed in that moment to be okay.
If you switch, it’s okay. It’s what you needed in that moment.
If you had no issues during the appointment but had fallout later, know that that’s common and you’re not alone.
If it went swimmingly, celebrate it. Littles almost always love celebrations :)
Be gentle with yourselves for the remainder of the day. If you need to chill and watch Netflix, let yourself. If you need to snuggle a stuffy and read, do that. Do you need to connect with another system who just “gets it?” Do that. Do whatever it is that truly takes care of you.
Perhaps someday, TIC will be something that every provider everywhere has down and does well. Until that day, we can continue to develop strategies to get through challenging appointments. We can connect with each other in the DID community, and share what works well with each other, in order to help each other through these challenging moments. After all, we are stronger together.
Thank you for being here!
It is important to avoid confusing Trauma Informed Care with Trauma Treatment or Trauma Therapy-they are very different things.