

The Simple Complexity of Treating DID
The Simple Complexity of Treating DID
Thoughts From a Therapist With DID


We love learning. In fact, we are almost always engaged in a course, webinar, book or something designed to further our knowledge and skillsets. In the past couple of years we’ve been particularly devoted to learning more about treating complex dissociation, DID in particular. If you’re wondering, “But y’all have DID! Why ya gotta learn about it?” It’s because we are just one system, and, as the saying goes, if you’ve met one system, you’ve met one system. What works for us has no guarantee of working for, or even remotely helping other systems. Learning as much as possible paired with critical thinking and empathic attunement skills increases our chances of being truly helpful to other systems and their providers.
When we systems seek care, so many of us are met with, “I’m sorry, that’s out of my wheelhouse. I don’t treat that.” It’s so disheartening and unfair to hear that time and again. It leaves us feeling like we’re “too much” or “too broken.” Yet, neither of those things are true! All systems have unlimited capacity for healing, transformation, change and thriving in the world. (And don’t ever let anyone tell you any differently!)
On the one hand, it has been remarkably encouraging to see the number of clinicians in the courses we’ve taken, all eager to learn about DID/OSDD so they can provide competent care to folks who have these conditions. On the other hand, we’ve noticed that many of these clinicians are seeking prescriptive treatments and methodologies. In other words, they’re asking for “exactly” how to treat clients with DID and OSDD. “How do I use CBT to treat it?” “What do I do first?” “How do I use DBT to treat it?” “Why isn’t IFS perfect for it? How can I adapt IFS, because it’s what I’m trained in.” “How do I use EMDR with systems? I’ve heard you’re not supposed to.” (Spoiler alert: EMDR can be used with systems) “Do I talk to each and every part??” (Hint: Talk to the ones that present and make sure all know they are welcome.)
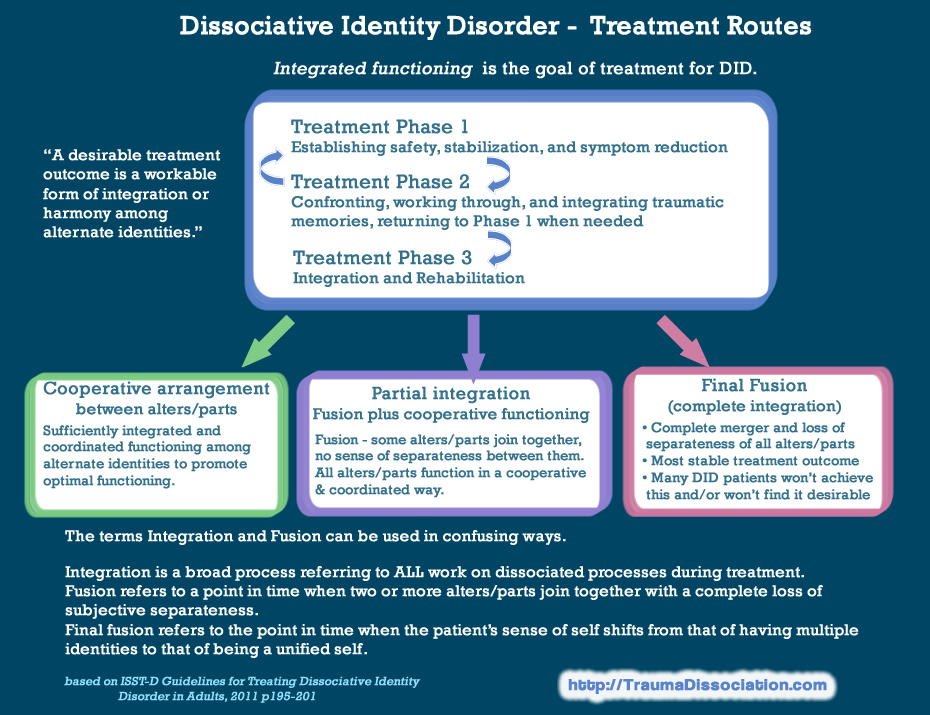
The reality is, there is no one specific way to provide care for clients who are systems. Remember: if you’ve met one system; you’ve met one system. There is a brief ‘roadmap’ in treating people who have DID/OSDD. Leading experts in the field describe a triphasic approach where Phase I is establishing safety, stabilization and working to reduce troubling symptoms. Phase II is working through traumatic material and returning to phase I whenever it's warranted. Phase III is integration and rehabilitation where a system may stabilize in functional multiplicity, final fusion or some combination of the two.
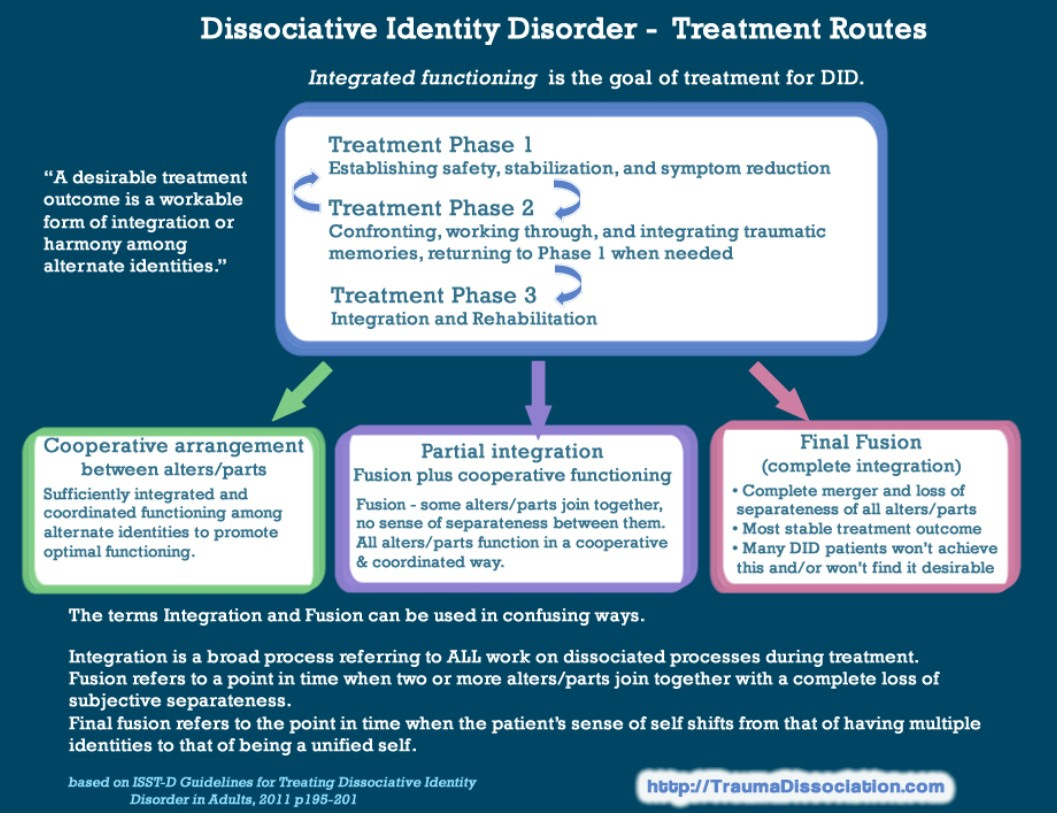
You’ll notice that in those three phases of treatment, there is no mention of specifically how those things are accomplished. That means that we, as clinicians, need to use a combination of tuning into our clinical intuition, compassionately attuning to and listening to our clients while closely observing their responses and then seeking consultation when needed, in order to guide the therapy, including the choice of modalities and interventions for each and every individual client we treat. When asked which modalities are best to use for treating DID/OSDD, Dr. Jamie Marich, a highly regarded expert in the field, who herself identifies as being a system, often responds with, “none of them…and all of them.” Simply stated: It depends on the client.
So, why then, when there is a ‘roadmap’ of triphasic care and permission to use sound clinical judgement, do we think there is such insistence on learning the “exact way” to treat complex dissociative disorders?
Well…probably lots of very understandable reasons. Some examples are:
Clinicians fear accidentally causing harm to vulnerable individuals.
Clinicians are afraid of “doing it wrong.”
Clinicians worry that: “I don’t know what I’m doing.”
Clinicians fear that clients won’t get better in therapy or may even get worse.
If this happens, therapists then worry about what that says about their skills as a therapist. “Do I suck at this job that I love so much??”
Some clinicians believe there is only “one right way” of doing treatment for specific disorders, and if they are not “following the rules” they become anxious.
Clinicians are afraid to ‘experiment,’ often forgetting that clients teach us what we most need to know about what they need and what to do with and for them.
Some clinicians fear being transparent and authentic with their clients.
In general, clients who are systems tend to demand a level of authenticity that many clinicians are uncomfortable with. We have a sort of keen radar, if you will, that can sense when someone is being disingenous from miles away.
Some clinicians worry that they will not be able to “get a client back” if the client dissociates to a certain degree.
So, you see, fear is usually the biggest driver behind the insistence of prescriptive methods of treatment. Yet, there will never be a manual that can dictate every step of treatment in the order they need to be taken that will work for every individual. That’s true of any diagnostic category, not just DID/OSDD.
{kind=link}
So What Am I Supposed to Do???
If you’re a clinician, “what am I supposed to do?” may be the question that has been swirling in your mind for a while now. The answer is as simple as it is complex: use the good clinical intuition you have, empathically attune to your client, be curious, and feel your way through it. Notice what resonates with your client and what doesn’t, and adjust what you are doing accordingly.
Remember, too, that according to The Heart and Soul of Change, about 50% of change is attributable to the client, 30% is attributable to your relationship with your client and only 12% is attributed to the actual modality or intervention you choose to use. According to other sources, the remaining 8% is attributed to the level of hope clients and the therapist have. When you look at those statistics, exactly what you do in terms of intervention is not particularly influential in the overall outcome. In fact, if everything goes right, your intervention can flop entirely and your client can still make progress and heal. We’re reminded of the sage words of one of our Clinical Practice professors in grad school: “Before you get all upside down, you all need to know that you’re not going to save anyone. You’re also not going to kill anyone. Your clients survived before you and they’ll survive when you’re not there.” As an aside, she was also the same professor who wisely advised her classes that, “Sympathy is located between shit and syphilis in the dictionary. Don’t ever have sympathy for your clients, it’s demeaning. Always have empathy for your clients. There’s a big difference. Don’t ever forget that.” To be sure, it was unforgettable advice.
Therapy can, of course, go south. For a while, our system worked with a therapist who was purportedly an “expert in treating DID.” She had seemingly all the right qualifications and experience. She’d done it all before, many times, with clients who had DID. She was trained and certified in EMDR, Sensorimotor Psychotherapy, hynposis and IFS (arguably we were less excited about the IFS component). She had been in peer consultation groups with some big names in the trauma field. She even worked in Bessel van der Kolk’s Trauma Clinic… she did all the things. What she did not do was compassionately attune to us, stay present and feel her way through our care. The disconnect was gaping and ultimately the relationship crumbled, unable to be repaired, leaving us in the unenviable position of having things opened up with no safe enough place to rest. The moral of that story? All the skillsets and tools in the world are useless without the ability of the therapist to be authentically present, empathically connected to the client and able to compassionately respond.
So, therapists… the answer of what to do is, again, as simple as it is complex: Breathe, trust yourself, relax into the process, be curious, attune to your client with compassion and respect, listen carefully, feel your way through it, ask for feedback, and seek consultation as needed. Most of all, believe in your clients’ capacity to heal…because, unquestionably, it is there.