

Having a Voice
Having a Voice
Unpacking the McLean Video and Finding a Path to Healing

Imitative DID is Not the Real Issue Here…
It’s been about 3 weeks since the presentation on “imitative DID” rocked the plural community. We don’t know about you, but we find ourselves still thinking about it, still bothered by it. In fact, the reason that this writing is so late in coming is that we’ve actually started it several times. So…What is it about the presentation that disturbs us most?
To be clear, the suggestion of and focus on “imitative DID” isn’t the problem. After all, questions of “faking it” come up plenty, including internally for most of us who have the diagnosis. If you have a DID/OSDD diagnosis, you’ve probably also asked yourself: “Am I making this up?” a multitude of times. The topic of ‘imitative DID’ isn’t new or innovative.
In fact, there are others who have done a great job at explaining indicators that point to when someone might be feigning DID. Two years ago, Jess, who managed the popular Multiplicity and Me YouTube channel, created a video titled Factitious/Fake DID: The Expert Checklist that got 476,000 views, 19,000 likes, and, from what we can tell, generated no controversy whatsoever. She was compassionate, clear, and concise in her synopsis of the 12 flags most experts look for to differentiate bona fide DID from factitious DID. Her explanation even garnered praise from UK expert Dr. Mike Lloyd who commented: “
Thank you for this, Jess. It will be extremely helpful going forward in raising awareness and training professionals in correct diagnostic skills. Very well balanced, drawing on key research and offering insight from your own perspective. This will become a key video to point people towards when they doubt their own diagnosis. Clinically, my experience is seeing people with DID who do not hit these flags, and helping those people understand what DID is through expert-by-experience is critical, so your educational videos help enormously. Keep up the good work!
The primary article Jess referred to was Factitious and Malingered Dissociative Identity Disorder, originally published in the Journal for Trauma and Dissociation in 2001. The 12 clinical features (red flags) it identifies as suggestive of malingering or factitious DID are:
Having a score above 60 on the Dissociative Experiences Scale (DES)
Reporting dissociative symptoms inconsistent with the reporting on the DES
Being able to tell a chronological life story and to sequence temporal events
Using the first person over a range of affect
Being able to express strong negative affect
Bringing "proof of a dissociative diagnosis to the consultation
Having told people other than close confidants about the alleged abuse or alleged dissociative diagnosis
Reporting alleged abuse that was inconsistent with the medical or psychiatric history or volunteering allegations of cult or ritualized abuse
Telling of alleged abuse without accompanying shame, guilt, or suffering
Having been involved in community self-help groups
Not having symptoms of co-morbid posttraumatic stress disorder
Having obvious secondary gain in having a dissociative diagnosis
In the notes, Jess also cited Assessment of complex dissociative disorder patients and simulated dissociation in forensic contexts by Brand, Webermann & Frankel (2016) to support the postulation that there are indicators that can differentiate between ‘real’ and ‘feigned’ DID. She is also careful to cite the article, Iatrogenic dissociative identity disorder—An evaluation of the scientific evidence by Brown, Frischholz, & Scheflin (1999) which debunks the idea that “major psychiatric diagnosis like dissociative identity disorder per se can be produced through suggestive influences in therapy,” clarifying that, “some scientific evidence exists to show that behavioral reinforcement can affect the frequency and type of alter behavior manifesting in patients who already have DID.”
The Importance of Having a Voice
So, again, it’s not the suggestion that people might purposefully mimic DID that is the problem. That happens. We all acknowledge that. So, what was so egregious about this presentation? Well… A few things.
One of the most challenging aspects is the aftermath of silence itself. It mimics the trauma and abuse that so many in the plural community have already suffered. A white male in a position of undeniable privilege and authority at an elite academic affiliated hospital created and gave a presentation that harmed specific, identifiable, vulnerable individuals. The aftermath of silence is reminiscent of the culture of abuse itself: “What happened was wrong, but don’t talk about it and let’s move on as if nothing happened.” This dynamic increases suffering, intensifying the egregiousness of the event. Healing, by nature, often necessitates that we have a voice.
Like many professionals and people in the community, we have reached out with an invitation for a robust discussion that could illuminate ideas to mitigate damage and find a healing path forward. Not surprisingly, the request went unanswered. Because everyone deserves a voice and verbal expression assists healing, we’ve decided to have a voice and do a little unpacking here with you. We hope that what follows feels validating to each of you reading it, and perhaps, Dr. Robinson will be so inclined as to read it privately and reflect on the following points:
Unpacking the Harm
1. Good Intentions: It is likely that Dr. Robinson had good intentions in creating and delivering his presentation. Perhaps he truly desired to help professionals better sift through complex diagnostic pictures to arrive at diagnoses that could better guide their treatment decisions. However, present-day social justice movements posit that intentions are irrelevant when harm is the result of actions. Instead, the focus must be on the actual impact of and accountability for the harmful actions taken. The impact of those actions is illustrated in the remaining issues that follow.
2. Unacknowledged privilege: As a cisgendered, white male in a professional position of authority, Dr. Robinson enjoys tremendous privilege and power. Viewing the world through a lens of such privilege, without acknowledging its existence, is problematic at best. He is employed by an elite, Harvard affiliated psychiatric hospital purporting to deliver world class treatment that is not accessible to everyone. Socioeconomic and geographic barriers prevent many people from accessing care at McLean. Even economically privileged individuals, who can either pay privately or afford their insurance mandated cost share, are placed on challenging waitlists due to census and staffing capacity. Access to his private practice, which does not accept insurance, is also greatly limited. By default, then, he primarily works with individuals who enjoy privileges like those that he enjoys. This means that, his data is driven by the sampling of individuals he treats and referenced in his presentation. Those people are not necessarily representative of the totality of individuals who experience dissociative disorders. Yet, his presentation strongly implied, and made it easy to infer, that he somehow has experience with all iterations of symptom pictures housed within the DID diagnostic label. He did not acknowledge other presentations of the disorder that deviate from the individuals he has treated, such as the previously mentioned and respected Jess of Multiplicity and Me. Instead, he heavily implied that any variation from his patients must be “imitative” and, by default, invalid.
Furthermore, he failed to acknowledge that not everyone has access to professionals to seek an evaluation or diagnosis from. Until there is equity in healthcare that creates access for all people to seek professional assessments for diagnostic clarity, people will continue to seek information that is both free and widely available online. Most people can critically evaluate the information they find online and subsequently use it to improve the quality of their lives. This is a good thing.
3. Ethics & The Use of Disclaimers: Dr. Robinson is careful to note at the outset of his presentation that the clips he used are for “illustrative purposes only” and that “I don’t claim to know anything about the individuals portrayed, beyond what they share freely and publicly online.” In effect, he is saying, “Since this is posted online, I can use it in whatever way I wish, and since I note that I do not know these individuals, I can portray them in disparaging ways without recourse.” There are several problems with this.
a. Dr. Robinson is a doctoral level psychologist bound by a clear Code of Ethics as set forth by the American Psychological Association (APA). Section 8.03 of the APA Code of Ethics states:
Psychologists obtain informed consent from research participants prior to recording their voices or images for data collection unless (1) the research consists solely of naturalistic observations in public places, and it is not anticipated that the recording will be used in a manner that could cause personal identification or harm, or (2) the research design includes deception, and consent for the use of the recording is obtained during debriefing.
While we understand that this presentation was not a specific research project per se, it was presented as educational related to research he has engaged in. The content creators’ faces and social media handles were all prominently displayed, making them easily identifiable to anyone who viewed the presentation. While the individuals whose content he used were public, and, therefore, one could argue that the personal identification was irrelevant, it is imperative to note that the section also mandates that he guard against using the recording in a manner that could cause harm. He failed to do this.
b. Additionally, the Code of Ethics Competence Section 2.01(e)
States: In those emerging areas in which generally recognized standards for preparatory training do not yet exist, psychologists nevertheless take reasonable steps to ensure the competence of their work and to protect clients/patients, students, supervisees, research participants, organizational clients, and others from harm.
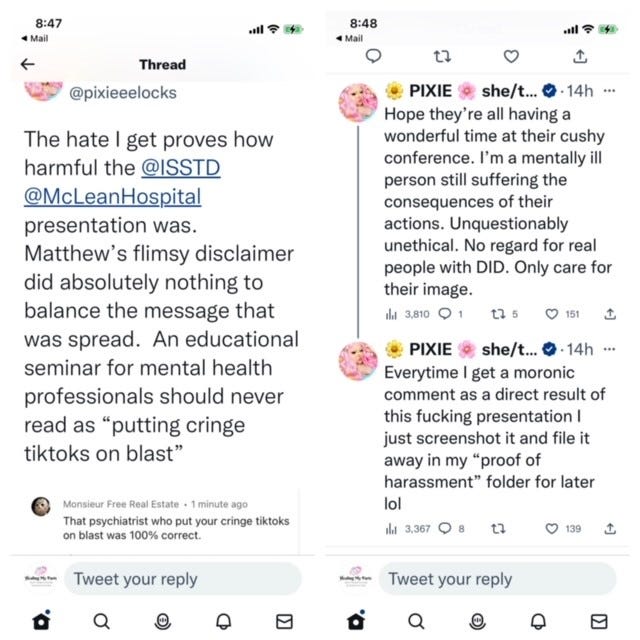
When practicing, teaching, researching and conducting ourselves in any professional capacity, it is standard practice for any mental health professional to protect others from harm. In fact, most mental health professions’ Code of Ethics include that as an integral expectation of ethical practice. We encourage Dr. Robinson to navigate back to the pages of the accounts he used in his presentation. They have all spoken out about the harm they suffered and continue to suffer as a direct result of his use of their material. Undeniably, he harmed the very people he is tasked with protecting. Stating “Again, I don’t know anything about these individuals except what they’ve put online,” does not protect against harm nor has it mitigated the damage done to them. To date, there has been no public acknowledgement or accountability for this harm.
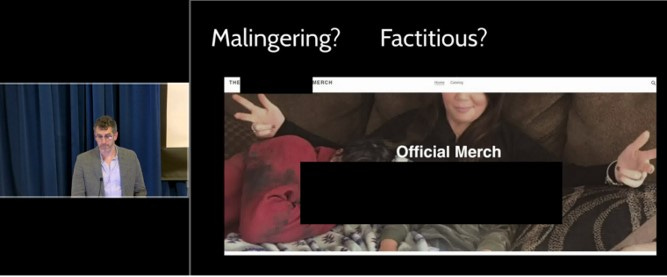
c. Despite the initial disclaimer that, “I don’t claim to know anything about these individuals portrayed, beyond what they have shared publicly,” he proceeded to use each clip as an example of “imitative DID.” In fact, in one slide he shared a picture of an individual with their social media handle and face clearly displayed, and added the words “Malingering?” and “Factitious?” directly above the picture. This depiction clearly implied that he believes that the individual suffered from either Malingering or Factitious Disorder and not “genuine” DID.
When we return to the specific APA Code of Ethics that he is bound by, Section 9 defines ethics regarding assessments of individuals.
Section 9.01(a) Psychologists base the opinions contained in their recommendations, reports, and diagnostic or evaluative statements, including forensic testimony, on information and techniques sufficient to substantiate their findings. (See also Standard 2.04, Bases for Scientific and Professional Judgments .)
(b) Except as noted in 9.01c , psychologists provide opinions of the psychological characteristics of individuals only after they have conducted an examination of the individuals adequate to support their statements or conclusions. When, despite reasonable efforts, such an examination is not practical, psychologists document the efforts they made and the result of those efforts, clarify the probable impact of their limited information on the reliability and validity of their opinions, and appropriately limit the nature and extent of their conclusions or recommendations.
(For reference 9.01c states: (c) When psychologists conduct a record review or provide consultation or supervision and an individual examination is not warranted or necessary for the opinion, psychologists explain this and the sources of information on which they based their conclusions and recommendations.)
The viewing of brief clips on TikTok clearly does not constitute an examination sufficient to render a diagnostic opinion. Yet, he held each of these individuals out as having “imitative DID,” Malingering or Factitious Disorder. These are individuals who shared that they were diagnosed by professionals as having Dissociative Identity Disorder. The rudimentary viewing of a TikTok video is neither robust nor thorough enough to nullify the diagnosis given by professionals who evaluated their individual clients in person. Thus, his presentation both directly harmed the individuals whose videos he shared and discredited the professionals who treat them. This appears to be a direct violation of the Code of Ethics he is bound by.
4. The Role of Shame: Throughout the presentation, Dr. Robinson focuses on the intense shame, embarrassment, and confusion people with ‘genuine’ DID experience. We do not dispute that this is a ubiquitous experience for those of us who have DID. However, shame, embarrassment and confusion do not necessarily have longevity for everyone with the disorder. Very often, at the onset of treatment, shame, embarrassment and confusion are pervasive. As people heal and come to appreciate the brilliant, creative way their minds secure their survival through unfathomable trauma, the shame and embarrassment tend to lessen. As people develop internal communication, cooperation and collaboration with their parts, confusion begins to fade. Additionally, shame can be greatly mitigated by meeting others who share the same diagnosis and have similar experiences. The Healing Together Conference, partially a McLean sponsored event, is one such example that helped to lessen some of our personal shame and embarrassment. Perhaps his experience is limited to only those who are at the beginning of their healing? Perhaps he has never witnessed a client feel compassion and love toward their parts? If so, we find that profoundly sad.
5. Plurality or Multiplicity: As Dr. Robinson discusses endogenic plurality, he brings up the topic of plural pride and multiplicity being integral to people’s identity, noting that in traumagenic presentations, “people with DID don’t choose this, they don’t wish for this.” This is problematic for a couple of reasons. Firstly, it suggests that there is something wrong with having pride or striving for functional multiplicity. Secondly, final fusion does not appear to be possible for everyone with traumagenic DID/OSDD. Thirdly, once people get to know their parts and feel compassion for them, not everyone wants final fusion. Functional multiplicity is a valid goal and a valid treatment goal. Suggesting otherwise is irresponsible and creates undue confusion and suffering for those who experience dissociative identities.
6. Iterations of Diagnostic labels: Dr. Robinson’s lecture strongly suggests that there is only one presentation of ‘genuine’ DID: a shame-filled, embarrassed, confused and very secret one. While the majority of systems are covert and switching is easily missed by others, some systems are, in fact, more overt. Again, we turn to the example of Jess, from Multiplicity and Me. Jess is public, widely respected and was part of an overt system. They were featured on television and dedicated a significant portion of time to educating others about DID through their popular YouTube channel. Nuance and multiple iterations of symptom pictures do exist within the DID diagnosis. This was not conveyed by the presentation, and therefore, did a grave disservice to professionals and clients alike. We have already heard professionals who have watched this presentation readily dismiss some overt presentations as “imitative” without in depth investigations. This is tragic for the clients who are readily and summarily dismissed based on solely on this lecture. The ripples of this presentation will create a legacy of harm that will be far reaching.
7. Neurodiverse Youth and Stigma: Dr. Robinson also stated (we are paraphrasing here) that the influx of people he is seeing, who are referred for assessments for DID, tend to be Neurodiverse (ND) youth seeking a diagnosis for “connection and attention from their family and friends.” He cites is their use of professional jargon as an indicator of imitative DID. However, youth today are far more open about their mental health struggles than previous generations have ever been. They talk freely about a host of mental health issues with each other both in person and online. Youth today also spend significant amounts of time online consuming media and researching information about their struggles. It is not necessarily surprising, then, that they have a good command of professional jargon. This fact does not necessarily negate a diagnosis. Furthermore, he also identifies “obvious switching” as a red flag of imitative DID. For some systems, overt switches do occur in safe settings. It is not inconceivable, given the drastic change by how mental health is viewed by younger populations, coupled with the likelihood that they would assume that a professional experienced in treating DID would be, by default, safe. Given these circumstances, they just might feel safe enough for their system to present overtly in the presence of that assumed safe professional. Lastly, we would be remiss to not underscore that specifically targeting ND youth only serves to further marginalize that particular already oppressed population.
In Conclusion
So, yes, there are multiple problems with Dr. Robinson’s presentation. Again, it is not the suggestion of “imitative DID,” but rather the fact that certain identifiable individuals were harmed and continue to be harassed, because a white, cisgendered, privileged male psychologist tasked with protecting vulnerable people chose to use vulnerable people’s content in a public, discrediting and disparaging way. Both he and McLean may choose to ignore this writing, falsely attributing the upset in our community to being “too emotionally attached,” since we live with DID. That would be a missed opportunity for them. Nevertheless, the above points stand on their own merit, separate and apart from any of our emotional experiences. We can heal from this experience by speaking out and sharing the truth while leaning on each other for support.
We sincerely hope that Dr. Robinson will take time to reflect and consider the ways in which his lecture violated ethics and harmed vulnerable people. At the very least, an acknowledgment and sincere efforts to do better in the future would be greatly appreciated by those feeling retraumatized by his actions and deafening silence.
Incredible article. You highlight such important points regarding ethics mental health providers must practice by and be mindful of in all of their work, including such public presentations that may and will impact many. You also validate the many iterations of DID/OSDD and especially validate that functional multiplicity/plurality is a worthwhile goal. Thank you for your work. Thank you for giving voice to our community.
Great job! Thank you!